Health policy-making is a human endeavor, and as such, is inextricably linked with the ethics of those involved (Longest, 2010). A lesson learned early on by nursing students are the ethical principles of autonomy, justice, beneficence, and nonmaleficence (Longest, 2010). Each of these pillars has its own place in the world of health policy, and can also be found in the political decisions which shape family planning policies in Arizona. However, rather than listing and defining these principles, which you are likely very familiar with, I would like to introduce a concept known as person-centered care (McCormack & McCance, 2017).

Person-Centered Care
Many healthcare providers will be familiar with practicing person-centered care, even if they have not labeled it as such in their daily work. The concept of person-centered care is explained by McCormack and McCance (2017) as a practice which treats people as autonomous individuals, while building trusting, therapeutic relationships. This concept emphasizes the importance of shared-decision making between a provider and their patient (McCormack & McCance, 2017). It weaves together the pillars of autonomy, justice, beneficence, and nonmaleficence and has been acknowledged by the World Health Organization (2015) as “an approach to care that consciously adopts the perspectives of individuals, families, and communities… [requiring] that people have the education and support they need to make decisions and participate in their own care.”
Person-centered care has grown in importance and recognition, and many countries throughout the world are making efforts to incorporate it into their healthcare systems (McCormack & McCance, 2017). It is a concept which McCormack and McCance (2017) argue should be integral to health policy-making, because our healthcare landscape today needs policies that put patients, families, and communities at the crux of decisions.
Justice in Family Planning Services
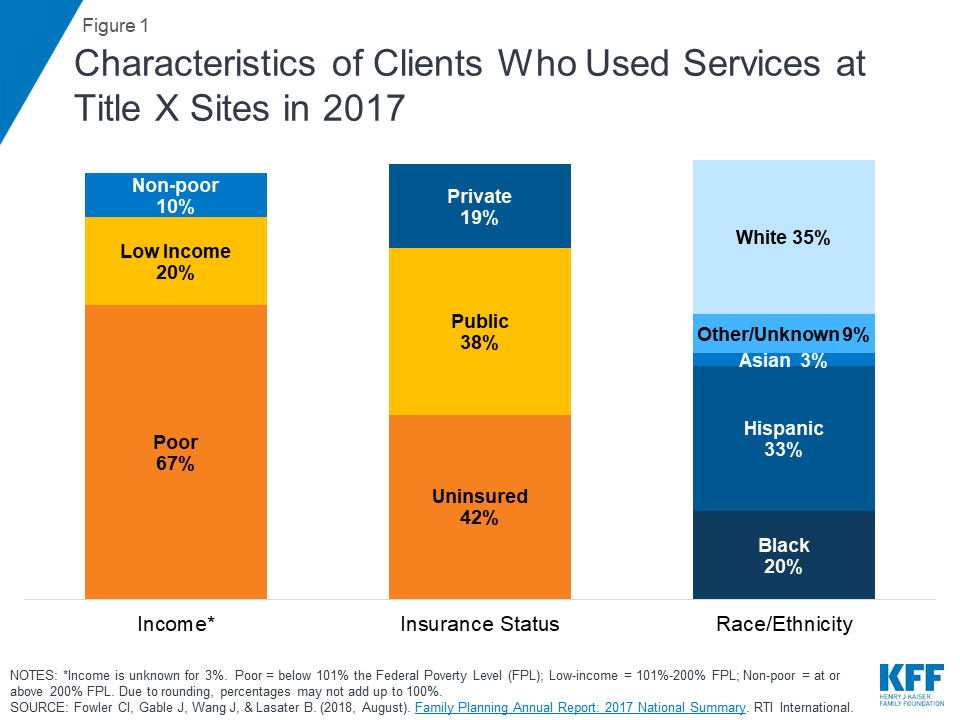
There are different perspectives on the concept of justice, which is why creating a person-centered health system does not come easily (Longest, 2010). An individual who holds an egalitarian view of the principle of justice would argue that healthcare resources should be equally available to all people (Longest, 2010). This involves understanding that people seek healthcare with different backgrounds and different needs, and that some patients may require more assistance than others (Longest, 2010). Supporters of government-funded family planning services, such as Medicaid and Title X funding, would subscribe to an egalitarian point of view in that they believe those who have less money should receive support from the government in order to receive the same care as those who have more money. The majority of patients who receive care under programs such as Title X are living at or below the poverty line (Sobel, Salganicoff, & Frederiksen, 2019). The patients that rely on these programs are among the most vulnerable in our communities, and it is our responsibility as healthcare providers to promote programs that will support them.
Reproductive Autonomy
The World Health Organization (WHO) (2020) emphasizes that it is a woman’s fundamental right to have access to reproductive health information and care, free from coercion. The principle of autonomy defends the right of patients to make their own choices after being given a complete and accurate description of their healthcare options (Longest, 2010). This principle also means that patients should have the right to choose who their healthcare provider is and where to receive care. Discussing family-planning options with patients involves a discussion of pregnancy timing, possible birth control options, continuation or termination of pregnancies, and other sexual health issues. These are all topics that women should feel safe and comfortable bringing up with their healthcare provider. However, the Gag Rule on Title X funded clinics has forced clinics that wish to provide comprehensive, bias-free care from withdrawing from the program (Sobel, Salganicoff, & Frederiksen, 2019). Rather than accepting the limitations put on clinics that are accepting funding from the Title X program, some clinics have chosen to decline funding and continue providing the comprehensive education and care they have always provided (Sobel, Salganicoff, & Frederiksen, 2019). Women who cannot pay for services without the assistance of the Title X program will be forced to find new healthcare providers, even though they may have built a trusting relationship with their current provider.

The Gag Rule which has been enforced on clinics receiving government funding for family planning services threatens the concept of person-centered care. It takes away the ability of providers to engage in shared-decision making with their patients, and erodes the trust that providers work so hard to build with their patients. When discussing such intimate and personal matters as sexual health and pregnancy, patients expect their providers to listen and respond with empathy and honesty, not to withhold information on resources because they are afraid of losing their jobs or funding for their clinic. What’s more, it interferes with the principle of justice as providing equal access to care for all. Women who rely on government programs to receive important health screenings, birth control, and obstetric care are put at a disadvantage when they cannot receive information on abortion when it is requested. It is not the place of the government to tell providers what they can or cannot discuss with their patients.
References:
- Longest, B. B. (2010). Developing competence in the policymaking process. In B.B. Longest Jr. (Ed.), Health Policymaking in the United States (pp. 181-216). Chicago, IL: Health Administration Press.
- McCormack, B., & McCance, T. (2017). Person-Centred Practice in Nursing and Healthcare: Theory and Practice. Oxford, UK: John Wiley & Sons.
- Sobel, L., Salganicoff, A., & Frederiksen, B. (2019,March 8). New Title X regulations: Implications for women and family planning providers. Retrieved from https://www.kff.org/womens-health-policy/issue-brief/new-title-x-regulations-implications-for-women-and-family-planning-providers/
- World Health Organization [WHO]. (2015). WHO Global Strategy on People-centred and Integrated Health Services: A Report. Retrieved from https://apps.who.int/iris/bitstream/10665/155002/1/WHO_HIS_SDS_2015.6_eng.pdf?ua=1&ua=1
- World Health Organization [WHO]. (2020). Abortion. Retrieved from https://www.who.int/health-topics/abortion#tab=tab_1

Your blog is a good start to advocacy about women’s reproductive rights. To be honest, I was completely unaware of this gag rule and or its effects. I was under the impression that abortion remained covered by insurances and was legal nationally.
However as you point out the gag rule, bans agencies to receive funding for counseling or referrals for abortion. Federally funded agencies must comply or risk losing funding altogether. This is unfortunate and places populations in vulnerable positions such as those who are; lesbian, gay, transsexual, bisexual, sex workers, and or young women primarily. Likewise, documented risks of not having access to abortion options are maternal death and unsafe abortions to name a few (N.A. 2019).
The concern is of the gag rule is that it does not foster health but focuses on political agenda. Likewise, you had voiced concern that the gag rule prohibits health rights and the ability to have complete conversations about reproductive health which could include abortion or counseling. My first impression when I read your blog was that Americans have freedom of speech, how is it that a provider cannot have a candid conversation with their patient if that is the desire of the patient. After doing some reading you are correct that the gag rule is followed out of fear. Providers are fearful about having that conversation and or documenting that advice when the risk is that all funding could be lost to their entire business/program.
Abortion is a difficult decision for a woman and many face judgment or criticism for this decision. Societal stigma is that abortion is bad and unattractive of a woman. Also, women face guilt and shame when in this situation and the gag rule would only make that existing problem worse (Frohwirth, Coleman & Moore, 2018). Imagine coming to the decision to that you are going to have an abortion and going to the doctor’s office to find out that they cannot talk to you about that option nor refer you to another provider or facility could help you with that need.
References
Frohwirth, L., Coleman, M., Moore, A. (2018). Managing religion and morality within the abortive experience: qualitative interviews with women obtaining abortions in the US. World Medical & Health Policy. (10) 4. Retrieved at https://onlinelibrary-wiley-com.ezproxy1.lib.asu.edu/doi/full/10.1002/wmh3.289.
N.A. (2019) The devastating impact of Trump’s global gag rule. Lancet. (393). 15-21. Retrieved at https://doi.org/10.1016/S0140-6736(19) 31355-8.
LikeLike
I had no idea that the Gag Rule on Title X funds had such far-reaching effects on underserved women! I had no idea that clinics accepting Title X funds could only offer natural family planning instead of all forms of FDA-approved contraception (Population Connection Action Fund, 2019). I remember the fundraising campaigns for Planned Parenthood, but I didn’t realize that the guidelines were so unbelievably strict. In addition, I didn’t realize that women who could only afford to go to a Title X clinic would need to change providers to maintain their health status.
This is the problem when policymakers put politics before people. However, the creation of government agencies and programs is how most countries in the world administer universal healthcare. The trick is to find a way to deliver safe, high-quality healthcare to patients and families that respects a patient’s autonomy. This is an increasingly difficult task in today’s society, especially as we grow more polarized every day.
Having attended my first Lobby Day at the Arizona Capitol, I saw firsthand legislators acting for the benefit of the people. I also saw legislators acting in their own self-interest. This is inherent in any profession, as long as human beings are involved. The key is to continue to advocate for the benefit of those who cannot advocate for themselves. This is our ethical and moral responsibility as healthcare providers who must give care to whomever needs it. In telling our stories and advocating for others, we can work together with policymakers to create positive change to improve access to healthcare.
References
Population Connection Action Fund. (2019). Title X and Trunp’s domestic gag rule. Retrieved from https://www.populationconnectionaction.org/title-x-and-trumps-domestic-gag-rule/
LikeLike
I so appreciate your posts. I am not familiar with many women’s health policies and I am learning a lot about Title X from your blog. I must admit that I am currently sitting in some tension with my feelings on the topic. While I agree with your comments regarding Title X Gag Rule threatening patient centered care, I think it is also important to define “patient”. The American Nurses Association states “the nurse’s primary commitment is to the patient, whether an individual, family, group, community, or population”1. While my intention is not to argue for or against abortion, I simply want to point out that the Gag Rule is perhaps laying foundation to protect a patient who is not yet seen.
I strongly agree with you that the Gag Rule is unethical as it removes a pregnant woman’s sense of autonomy and informed consent by not allowing her provider to discuss the full breadth of treatment choices. Where I was really astonished in reading up on Title X was how it prohibits providers from referring woman for abortions. While I believe that patients should be given the full range of treatment options so that they can make an informed decision, I personally would not advocate, perform, or promote abortion. The ANA also takes a similar stance in their position statement for when patients request medical aid in dying. Their position includes the nurse has “the right to conscientiously object to being involved in the aid in dying process”2. Instead of advocating, performing, or promoting abortion, I would simply refer my patient to someone who could. While I may not agree with her choice of treatment, I am professionally ethically bound to provide her with choices. Withholding referrals for one procedure would be unacceptable in any other aspect of medicine3. Referring her to someone who could advocate, perform, or promote abortion is how I can uphold both my professional and personal ethical guidelines.
Another reason I am against the Gag Rule is that many patients who currently receive care in clinics funded through Title X not only receive women’s health services but also primary care services such as treatment for hypertension, diabetes, or mental health3. If their clinic were to lose their funding, in reality these patients would lose so much more than just women’s health services.
References
1. American Nurses Association. Code of Ethics for Nurses with Interpretive Statements. Silver Spring, MD: Nursebooks; 2015.
2. The Nurse’s Role When a Patient Requests Medical Aid in Dying. Nursingworld.org. https://www.nursingworld.org/~49e869/globalassets/practiceandpolicy/nursing-excellence/ana-position-statements/social-causes-and-health-care/the-nurses-role-when-a-patient-requests-medical-aid-in-dying-web-format.pdf. Published 2019. Accessed February 9, 2020.
3. After Title X Regulation Changes: Difficult Questions for Policymakers and Providers. Healthaffairs.org. https://www.healthaffairs.org/do/10.1377/hblog20190923.813004/full/. Published September 24, 2019. Accessed February 9, 2020.
LikeLike