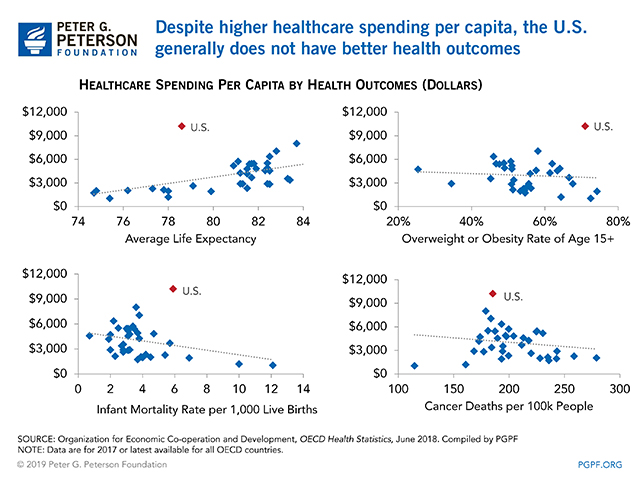
If there is one thing that can get always get people’s attention, it’s money. The U.S. is one of the highest spenders in the world when it comes to healthcare, with approximately $3.5 trillion spent in 2017 (Peter G. Peterson Foundation [PGPF], 2019). The cost of healthcare in the U.S. is continually growing (PFPF, 2019). In 1960, healthcare accounted for 5% of the Gross Domestic Product (GDP) of the U.S., and in 2017, it was up to 18% (PGPF, 2019). Reasons for this include a population that is growing older (16% of the population of the U.S. was over the age of 65 in 2017) and healthcare that just continues to increase in cost (PGPF, 2019). However, if a country has good health outcomes, spending a lot of money on healthcare may be justified. Unfortunately, this is not the case in the U.S., which significantly falls behind other developed countries in healthcare outcomes (PGPF, 2019).
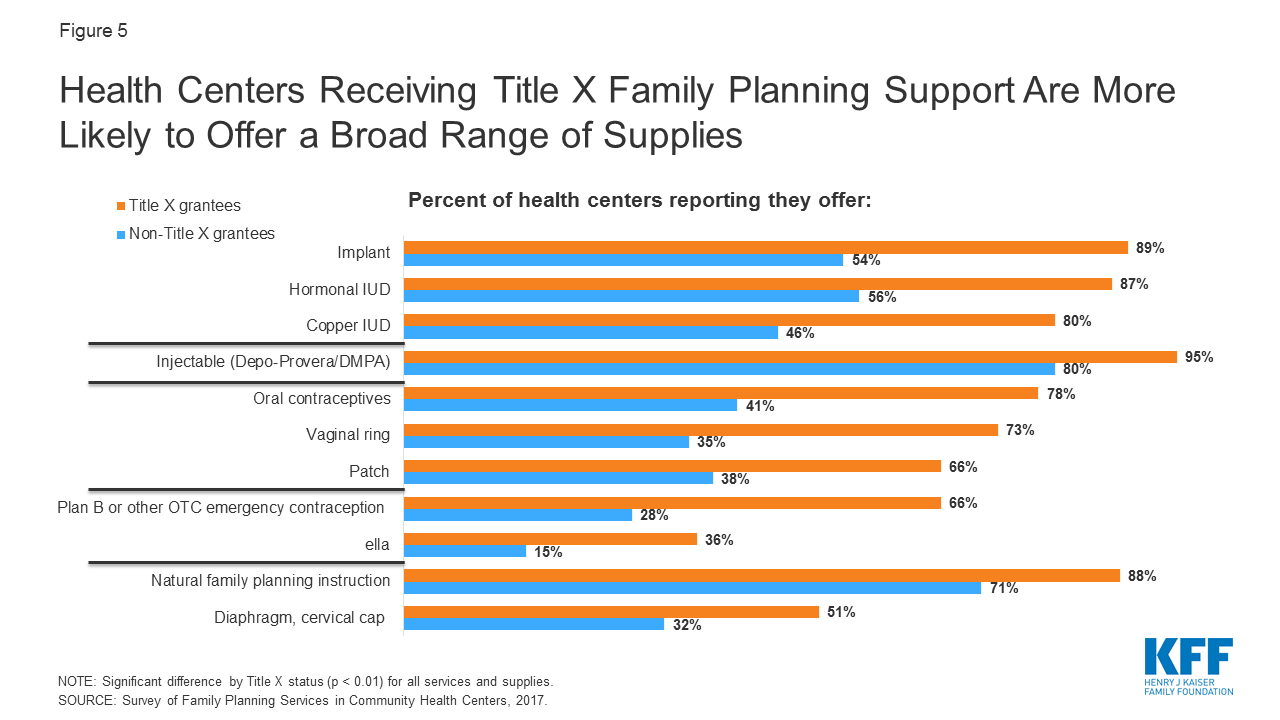
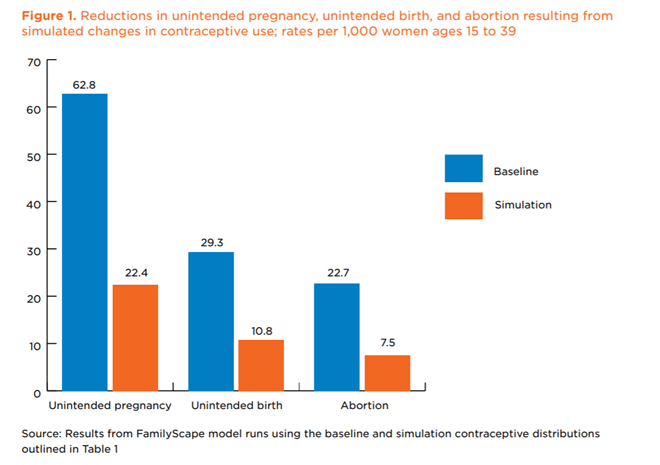
As healthcare providers, we must advocate for healthcare policy that emphasizes prevention and health maintenance, rather than the treatment of illness. One of the most important ways to do so is by advocating for family-planning and comprehensive women’s health services. Studies have shown that effective family-planning programs, and their subsequent increase in access to birth control, save billions of dollars for healthcare industries (Welti & Manlove, 2017). Unintended pregnancies can cause negative health sequelae for patients and their children, especially among women who have pre-existing health conditions which make pregnancy dangerous (Welti & Manlove, 2017). A research simulation in which every woman who was not desiring pregnancy in the U.S. had access to highly effective birth control estimated that there would be a 64% reduction in unintended pregnancies and a 67% reduction in abortions (Welti & Manlove, 2017). This ended up being a cost savings of $12 billion annually to the U.S. healthcare system (Welti & Malove, 2017). Just imagine if we could incorporate universal, effective birth control into our healthcare. We could drastically improve health outcomes for women who experience unintended pregnancy and decrease healthcare costs.
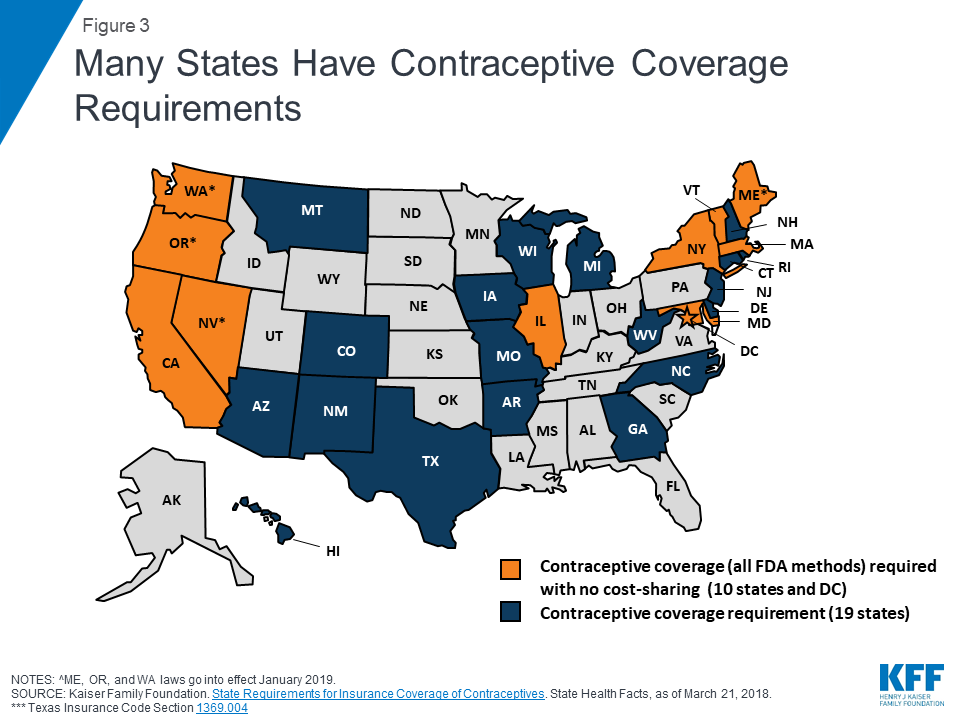
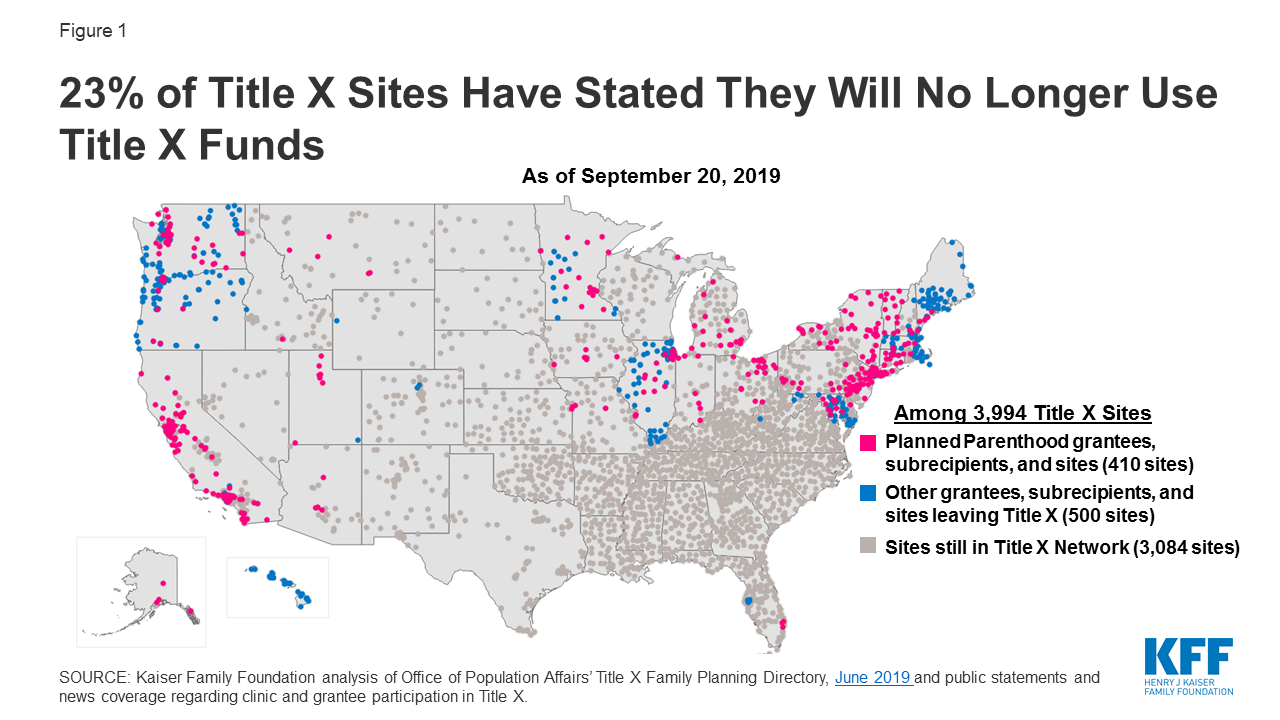
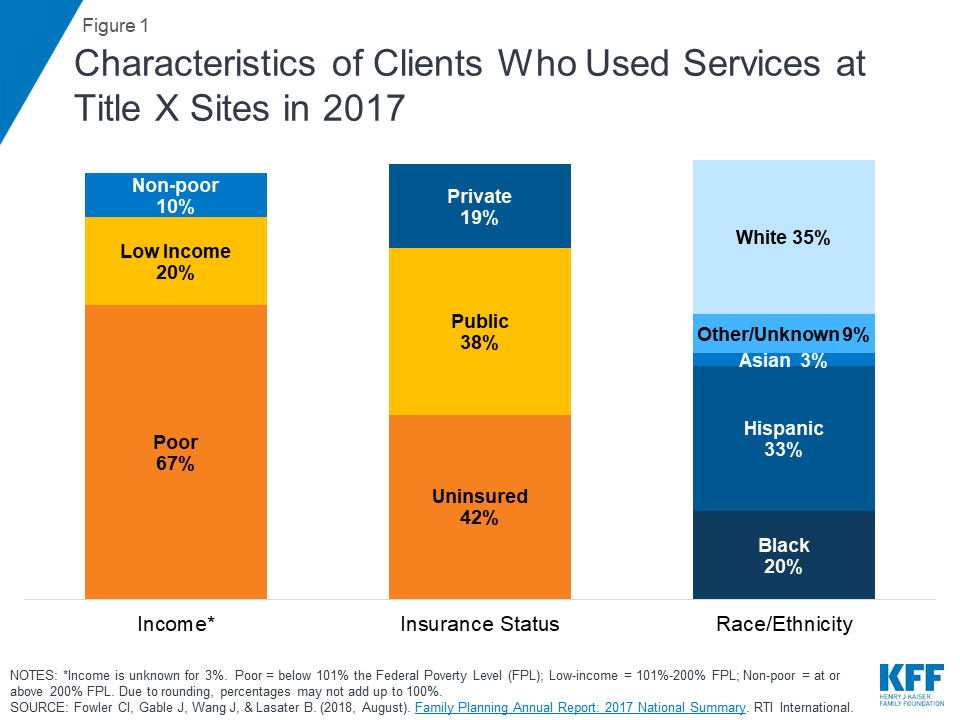
The sustainability of these solutions has already been shown by the substantial number of years family-planning services have been provided by government funded programs. The U.S. government has been providing family-planning services to low-income women for over 50 years (Ranji, Salganicoff, Sobel, & Gomez, 2019). With only one-third of low-income women using government programs to get their contraception, the availability of these programs is either not being communicated clearly enough, or is not widespread enough to reach the majority of women (Ranji, Salganicoff, Sobel, & Gomez, 2019). If all low-income women knew about the resources available to them, and there were enough clinics being funded by Medicaid and Title X programming, the country would be one step closer to have universal access to contraception. The recent restrictions placed on Title X funding, covered in previous blog posts, have only brought us further away from this ideal world in which we could save billions of dollars a year on abortions and unintended pregnancies. Once the return on investment is realized from the implementation of policies allowing universal access to birth control, sustainability of these policies won’t be an issue. The billions of dollars a year that could be saved from expanding birth control access could be put to use for other healthcare needs.
Legislation in Arizona to make access to birth control more widespread has been promising in the last year. Senate Bill 1493 would allow pharmacists to dispense birth control to women 18 years of age and older without a prescription from a healthcare provider (S 1493, 2020). This is one example of how policies can be changed and adjusted to make them sustainable within the ever-changing healthcare landscape. Policy modifications take place when negative consequences of policies are realized, or when a potential for beneficial change is seen (Longest, 2010). Policy makers suggest revisions and modifications to policies very frequently, as evidenced by the changes made to Title X regulations in 2019. However, when the changes made to policies have negative impacts on patients and the entire healthcare landscape, there will surely come a time when they are noted to be causing more harm than good. Healthcare providers who are passionate about providing equitable access to family-planning care should continue to advocate for low-income women all across the country. The changes made in 2019 to family-planning services are the opposite of sustainable; there will come a time when policy makers realize that the reduced number of clinics available for providing contraception has created higher healthcare expenditures. Until then, please continue to use your voice to stand up for equitable access to care.
References
- Longest, B. B. (2010). Policy modification. In B.B. Longest Jr. (Ed.), Health Policymaking in the United States (pp. 147-180). Chicago, IL: Health Administration Press.
- Peter G. Peterson Foundation (PGPF). (2019, March 15). Why are Americans paying more for healthcare? Retrieved from https://www.pgpf.org/blog/2019/03/why-are-americans-paying-more-for-healthcare
- Ranji, U., Salganicoff A., Sobel, L., & Gomez, I. (2019, October 25). Financing family planning services for low-income women: The role of public programs. Retrieved from https://www.kff.org/womens-health-policy/issue-brief/financing-family-planning-services-for-low-income-women-the-role-of-public-programs/
- S 1493, 55th Legislature, 2020.
- Welti, K., & Manlove, J. (2017). How increasing the use of effective contraception could reduce unintended pregnancy and public health care costs. Child Trends. Retrieved from https://www.childtrends.org/wp-content/uploads/2017/03/2017-03IncreasingEffectiveContraception.pdf